Prevention
Diphtheria is an acute infectious disease. It is a very contagious and potentially life-threatening bacterial infection. Diphtheria was a common cause of death in children up until the 1940s . Because of immunisation of children the disease almost disappeared, but it has once again emerged in some areas of the world with poor immunisation rates. There are fewer than five cases of diphtheria a year in the United States.The bacteria that cause diphtheria are called Corynebacterium diphtheriae and Corynebacterium ulcerans. Some of these bacteria also produce a toxin.
 | |
| Children in Seattle receiving the very first vaccination (1940) |
Symptoms
- There may be NO symptoms.
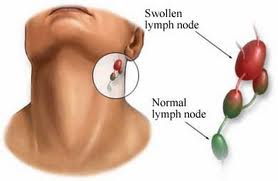
- Symptoms begin two to five days after exposure to the diphtheria bacteria. The first symptoms are usually a sore throat and a mild fever. A membrane forms over the throat and tonsils that can make it hard to swallow and breathe. The infection can also cause the lymph glands and tissues on both sides of the neck to swell. The bacteria most commonly infects the nose and throat. The throat infection causes a gray to black, tough, fiber-like covering, which can block the airways.
- A toxin formed by diphtheria bacteria can cause inflammation of heart muscle and nerves which can be fatal.
- Sometimes diphtheria can cause small skin sores that form larger ulcers, commonly on the legs. (generally seen in tropical areas)
- People usually take between two and five days to show symptoms after infection.
- Bluish colouration of the skin.
- Bloody, watery discharge from the nose.
- Breathing problems : Difficulty breathing, Rapid breathing, A harsh, high-pitched sound in inhalation or exhalation.
- Chills, fever, difficulty in swallowing, hoarseness.
- A croup-like (barking) cough.
- Drooling (suggests difficulty in swallowing).
 |
| Courtesty of Wrongdiagnosis.com |
How Do You Catch Diphtheria?
- Diphtheria bacteria can live in the mouth, nose, throat or skin on infected individuals.
- People with diphtheria are infectious for up to 4 weeks from the onset of symptoms. Some people may become carriers of the bacteria and so be infectious for longer.
- Corynebacterium ulcerans infection is occasionally associated with consumption of unpasteurised milk or contact with animals.
- Diphtheria spreads through respiratory droplets (such as those produced by a cough or sneeze) of an infected person or someone who carries the bacteria but has no symptoms. Diphtheria can also be spread by contaminated objects or foods (such as contaminated milk).
- People can also get diphtheria from close contact with discharges from an infected person's mouth, nose, throat or skin.

Those at Risk?
- Anyone who comes in contact with diphtheria during its infectious phase who has not had diphtheria in the past or has not been fully immunised is at risk.
 | |
| Throat membrane |
How Do We Prevent Diphtheria?
- Diphtheria vaccination protects against the disease. It is part of the standard vaccination schedule and is given as DTP vaccine, which contains combined vaccine against diphtheria, tetanus and pertussis.
- DTP vaccine should be given at 2,4 and 6 months of age, followed by booster doses at 4 years and at 15 years of age.
- A high vaccination rate in the community is important to protect the population from resurgence of this disease.
How Is It Diagnosed?
- A doctor can suspect diphtheria based on a clinical examination when the membrane is seen in the throat, and by testing throat swabs in a laboratory.
- Special laboratory tests are needed to detect the toxin and confirm the diagnosis.
- You may need an ECG (electrocardiogram).
 | |
| Skin lesions on throat |
How Is It Treated?
- Diphtheria infection is treated with antibiotics and antitoxin. If the health care provider thinks you have diphtheria, treatment should be started immediately, even before test results are available.
- Fluids by IV, Oxygen, Bed rest, Heart monitoring, insertion of a breathing tube and correction of airway blockages.
Diphtheria antitoxin is given as a shot into a muscle or through an IV (intravenous line). The infection is then treated with antibiotics, such as penicillin and erythromycin.
People with diphtheria may need to stay in the hospital while the antitoxin is being received. Other treatments may include:
- Anyone who has come into contact with the infected person should receive an immunization or booster shots against diphtheria. Protective immunity lasts only 10 years from the time of vaccination, so it is important for adults to get a booster of tetanus-diphtheria (Td) vaccine every 10 years.
Those without symptoms who carry diphtheria should be treated with antibiotics.
The death rate is 10%. Recovery from the illness is slow.

Complications
The diphtheria toxin can also damage the kidneys.
Diphtheria Is A Notifiable Disease
From :U.S. National Library of Medicine - The World's Largest Medical Library, and Pubmed
No comments:
Post a Comment