There are several main methods which are used to circumcise an infant, and remember I am not talking about places like Africa where there is no real hygiene and they carry out mass circumcision - with dire results.
A warning if you are squeamish - some of the pictures are graphic.
The first one I will talk about is the straight out cutting method. This is probably having its death knell sounded, although religious practices still seem to require this method. There really doesn't seem to be a standard for which method of circumcision is used, although some countries prefer the Plastibell and some the Gomco Clamp.
The so-called "simplest" method appears to have varied little from the "traditional" operation. The foreskin is pulled forwards and gripped in a pair of clamping or crushing forceps, which are placed at an angle to match the slope of the back of the glans. The skin is cut off in front of the blades of the forceps, then the inner skin is pushed back and fastened, with stitches, to the outer skin on the shaft. In infants, the stitches are often not used. Their main purpose is to close off blood vessels, and crushing with the forceps is often enough to accomplish this. How complete the circumcision is depends upon how hard the skin is pulled forward before clamping. Making the cut while the skin is pulled over the glans provides a safeguard against removing too much. Much of the inner skin remains, so the scar, after healing, will be well down the shaft. It is usually rather irregular but very inconspicuous.
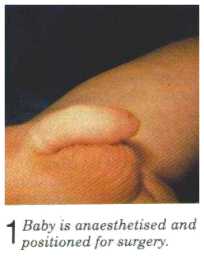 |
| NO ANAESTHETIC CAN BE USED |
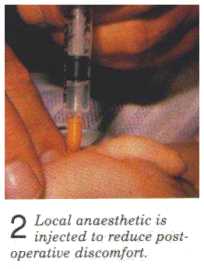 |
| Lidocaine is used. Note it is for after the operation. According to several nurses at University of Michigan, it does very little or nothing to alleviate the pain of circumcision. |
 |
| Betadine is used to swab the penis and scrotum to help prevent infection |
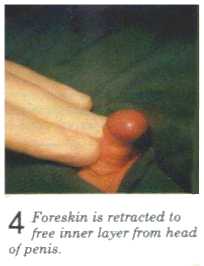 |
| The foreskin is sealed down to the penile head and must be torn off in order to be retracted in infancy. |
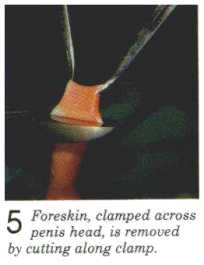 |
| The foreskin is pulled up, clamped for several minutes to prevent excess bleeding, and cut along the clamp with a scalpel. |
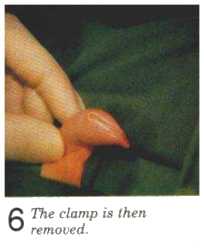 |
| What you see is not foreskin, but skin from the shaft of the penis. The edges stick together because they are still "raw". |
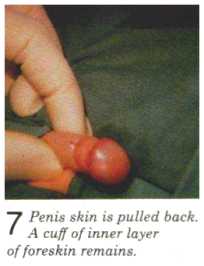 |
| The distinction between shaft skin and where the foreskin was cut away is obvious. The part of the foreskin that used to touch the glans ("inner foreskin") is what is between the shaft skin and the penile head in the picture |
 |
| Excessive bleeding is the most common complication of infant circumcision. |
 |
| After the inner foreskin is removed, notice that half the shaft skin has been cut away-- altogether,about 2/3 of all the skin of the penis. |
 |
| The remaining shaft skin is pulled up to meet the glans and attached with stitching. |
 |
| The penis now has 1/3 to 1/2 less penile skin to accommodate erections and the glans is permanently exposed. The glans will lose its shininess and dark red coloring as the site heals within the next week or so. What was before an internal part of the body, is now external and it will grow a sort of callous over the glans as part of the healing process. |
The Gomco Clamp, is an invention of Hiran Yelland and Aaron Goldstein, from 1934. It is reported to be based on the tyre lever used for Model T Ford cars. It is a metal ball, and a flat plate with a hole in it placed over both, to define the position. These are brought together by a screw and apply circular crush and fusing force - of between 8,000lbs to 20,000lbs.
Circumcision with the Gomco clamp and the Plastibell device have many of the same features. The foreskin is grasped with two mosquito clamps at the 10 o'clock and 2 o'clock positions These clamps are used to hold the foreskin up. A third mosquito clamp is used as a probe to destroy any adhesions under the foreskin from the 8 o'clock to the 4 o'clock positions and is then clamped about 2/3rd of the way between the foreskin opening and the corona. This action creates the crushed area for the dorsal slit. The third clamp remains in place for one minute. The dorsal slit is then cut through the middle of the crushed area, using tissue scissors. The foreskin is peeled back, and any additional adhesions are destroyed using a blunt probe.





The Gomco clamp was designed to crush about 1 mm of the foreskin around the circumference, while the Gomco bell protects the head of the penis from injury during removal of the foreskin. The bell is placed inside the foreskin, and the dorsal slit is secured over the bell with a sterile safety pin. This allows the handle of the bell to pass through the circular opening of the clamp, without the foreskin slipping out. The foreskin can be brought through the opening by grasping it with sterile gauze. The thumbscrew is tightened until snug, and the visible foreskin is removed using a scalpel blade distal to the junction of the bell and the clamp. The clamp should remain secure for a total of five minutes, to allow the crush effect to be complete. This step is designed to reduce the incidence of bleeding after the clamp is removed.
 |
| Gomco Clamp |
When the thumbscrew is loosened and the bell gently removed from the clamp, the foreskin will stick to the bell because of the crushing. The foreskin can be loosened by gently peeling with a gauze swab to liberate the glans and show the final result. The edge of the foreskin and the corona of the penis are then gently wrapped in precut petrolatum gauze, which remains in place for 12 to 24 hours.
The Plastibell is designed to cause circumcision by cutting off the blood supply to the end of the foreskin. Dead tissue falls off 7 to 12 days after the operation. No advantages of the Plastibell technique over other techniques have been documented, except "ease of use." Some studies have shown a small increase in the incidence of infection with the Plastibell device.



Ensuring that the correct size of the Plastibell is used is important. (N.B This is done by trial of different sizes) A fit too small can cause tissue strangulation and necrosis, and one too large may result in too much foreskin being removed and the penis being denuded of skin. After making the dorsal slit as outlined for the Gomco technique, the Plastibell device is placed on the glans and the cut foreskin is pulled over the top of it.
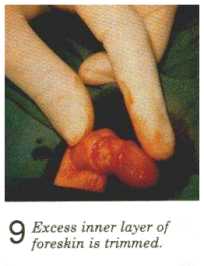
The cut foreskin is brought over the top of the Plastibell until the tip of the incision is above the string placement guide on the device. The foreskin is clamped across the top of the Plastibell with a straight clamp. The string is placed around the foreskin and the Plastibell device in a groove that acts as a placement guide. The string is then tightened and tied in a simple square knot. An adequate result is obtained when the skin just distal to the string blanches without the string breaking. The excess foreskin is trimmed from around the bell using iris scissors . The handle is then broken off the device.
 |
| Plastibell device |
The Mogen Clamp - A blunt-edged probe is used to separate the glans from the preputial lining, taking care not to traumatize the frenulum. The prepuce is lifted upward and outward by the hemostat. This action causes the glans to retract towards the scrotum, preventing accidental amputation of the glans. The open jaws of the Mogen clamp are placed around the prepuce (grooved side facing the glans) as it is lifted upward. The clamp is closed for one to one and one-half minutes. If the infant is more than six months old, the clamp should remain closed for five minutes.
 |
| Mogen Clamp |
While the clamp is closed, the prepuce is cut away distal to the clamp. The clamp is then opened slowly and removed. Downward pressure is applied to the skin around the corona, until the skin-mucosal seal is broken and the glans is liberated. A blunt probe is used to remove any additional adhesions. Petrolatum gauze is applied to cover the operative site. The preputial skin around the corona of the glans will often have a "dog-eared" or asymmetric appearance. As the infant grows, this aspect becomes less prominent.
There are other methods used, e.g. the Tara Clamp, the SmartKlamp. I believe the above will give you a fair idea of the procedure, without going into further clamp details.



Of course, the infant has to be restrained, and lo! there are manufacturers who have come up with the perfect solution. One of these if Olympic Medica's very own
Infant Immobilizer Circumstraint. Fast immobilization of newborns 4-16 lbs. Use during circumcision, transfusion, minor surgery, x-ray. Complete with four adjustable Velcro straps for securing arms and legs.
"In less than 30 seconds, a nurse can immobilize the struggling infant securely in the correct position with Circumstraint. It works on a proven principle of positive 4-point restraint. Soft wide Velcro straps encircle the infants elbows and knees, depriving him/her of leverage. "


"Circumstraint's comfortable contoured shape positions the infant, hips elevated, perfectly presenting the genitalia."
"He's held safely and securely without danger of escape."
"Always a fast, easy means of immobilizing newborns for circumcision..."

And the Stang
This light weight chair positions the infant comfortably while providing surgical access the the operative site."
"Newborn pain management is an issue
of concern to many health care
professionals today."
"Any physician or nurse who has attempted to extend the arms and legs of
a term neonate to strap him into a rigid restraint, realizes the
resistance to extension that all neonates possess.
Positioning of the
baby in the Circ Chair allows the infant to sit with his hips abducted
and flexed, knees flexed, and head elevated at various positions up to
30-45 degrees. Soft velcro straps adjust to the baby's size. The
instrument platform is designed to accommodate commonly used
circumcision clamps."
 | |
| The patient cannot understand, consent, refuse or escape. |
And the 'struggling infant' - hmm. No anaesthetic. Which I will cover in my next part of this blog, Part Three.